Saturday 02.04.22** at 14h BE
PICL, AAH, AAQC
2022 JAMA - Effect of Antiplatelet Therapy on SS and OSfd in CIpxs w_C19 (REMAP-CAP)
Sunday 10.04.22 at 19h BE
HIBN, AAQC
2014 CeCo - Boosting Vocabulary Learning By Verbal Cueing During Sleep (schreiner) [R].pdf
CW = cued words
UW = uncued words
1. Animal studies ➩ birds: sound learning IMP for development ➩ MAMAL ≠ BIRDS mechanisms of memory consolidation
2. SLEEP = IMP role in MEMORY CONSOLIDATION
3. ODORS + SOUNDS + MELODIES ➩ benefits ASSOCIATED MEMORY CUES consolidation ➩ HYPPOCAMPAL celss in rodents
4. RESULTS:
Sleep group ➩
- CW 105.14 ± 2.64%
- UW 95.43 ± 2.07%
Sleep control ➩
- CW 93.55 ± 2.37
- UW 92.80 ± 3.10%
Active awake
- CW 85.53 ± 2.8
- UW 84.2 ± 2.16%
Passive awake
- CW 79.86 ± 4.58
- UW 81.25 ± 2.09%
5. Sleep architecture NOT altered by cueing
6. ALL accompanied by distinct NEURONAL activities which involve sleep-specific slow oscillatory mechanisms.
7. Verbal CUEING ➩ efficient and effortless tool to ↗️ foreign vocabulary learning.
Saturday 16.04.22 at14h BE
LFMC, AAQC
2022 NEJM - Effect of Early Treatment w_ Ivermectin among pxs w_ C19 (Reis) [R].pdf
1. NO DIFF pOC and sOC for the 3 analysis ➩ intention-to-treat + modified itt + per-protocol
2. 3MA strongly benefit (different OUTPATIENT numbers) OTHERS NO BENEFIT
3. MA of trial ➩ iver DID NOT OFFER a TTO benefit
4. Well balanced covariates (iver VS placebo)
5. 2022, NEJM, BR ➩ db,adap,RCT ⏤ 3515 (679 VS 679) ⏤ Mar-Aug2021 ➩ P⃣ adults, sC19 + 1rf PROGRESSION I⃣ ivermec 400ug/Kg x3d C⃣ placebo O⃣ composed pOC: H+28 C19 or ED long stay >6h in 28d ➩ NO CHANGE
6. WHO ➩ very-low-certainty evidence ∑AGAINST use of IVER
Saturday 23.04.22 at 14h00 BE
LFMC, JJFM, AAQC
2022 JAMA - Association of Subcutaneous or IV Casirivimab + Imdevimab w_Clinical OC in COVID-19 (McCreary) [R].pdf
1. 2022, JAMA, US ➩ prospective ⏤ 1959 (969 VS 1306) + 2185 ⏤ Jul-Oct 2021 ➩ P⃣ 12 yo or >, sC19(+) ➩ PCR/Antg test, Symptom unknown EUA rf w_ no ED OR H+ I⃣ casirivimab + imdevimab SC C⃣ 1noTt, 2 casirivimab + imdevimab IV O⃣ pOC composed: H+28 OR MM ➩ casirivimab + imdevimab SC ↓ (vs noTt)
2. Only intravenous administration was evaluated in RCT. (IV strongly recommended by FDA)
3. REGEN-COV
4. POST HOC ➩ r_sH+ = ICU admiss OR MV
5. AdvEve = any reaction du_inj OR af_inj ➩ rash, shortness of breath, or HTA ⏤ secure electronic file–sharing APP
Saturday 30.04.22 at 14h00 BE
JJFM, LFMC, AAQC
2022 JAMA - COMET-ICE, Sotrovimab on Hº or MM hrPxs w_Mild to Mod C19 (Gupta) [RCT].pdf
1. 2022, JAMA, 57 sites (BR, CA, PE, ES, US) ➩ ph3_db_mcRCT ⏤ >1000 (<530 each group) ⏤ Aug2020-Mar2021 (ƒ-up Apr2021) ➩ P⃣ outPxs + SYMP <5d + mild-modC19 (rt-PCR or antigen) + 1rf_sDP I⃣ SOTRO 500mg/1h “1d” C⃣ placebo O⃣ pOC: ‘all-cHº>24h OR MM’_29 ➩ ↓ pOC , ↓ sOC 4/5 [COMET-ICE]
2. Predominant VOC were ∆ and Ω ➩ Jan2021
3. GREATER rf_sDP = older age, obesity, CKD
4. MechAction = targets HIGHLY conserved EPITOPE (the virus spike protein) ➩ does not compete w_ACE2
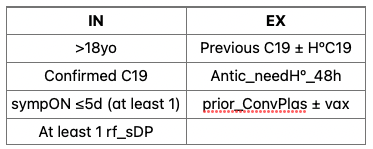
5. IN: a. ≥18 b. C19(+) RT-PCR or ANTIG c. SYMP <5d d. hr_sDP (1/7 rf):
- >55y
- DM w_med
- IMC >30
- CKD (GFR <60)
- CHF (NYHA II)
- COPD - ASTHMA mod-s
6. Stratification ➩ age (≤>70), duration SYMP (≤3d VS 4-5d), region (north VS -south America VS Europe).
7. FLU-PRO Plus questionnaire ➩ 32-item, no established MIN clinically IMP DIFF8. AdvEve ➩ infrequent + similar ➩ PLA = C19pneum 4% ⏤ SOTRO = diarrhea 2%
Saturday 07.05.22 at 14h00 BE
LFMC, AAH, AAQC
2021 NEJM - MOVe-OUT, Molnupiravir for Oral TTO of C19 in nHº pxs (Bernal) [RCT].pdf
1. 2021, NEJM, US ➩ db_pla_p-3_pg_RCT ⏤ >1400 (i716 VS c717) ⏤ May-Nov2021(f-up included) ➩ P⃣ outPxs, unVAX, mild-mod, lab-confirmed C19 I⃣ MOLNU 800mg BID 5d C⃣ PLA O⃣ pOC: EFF "Hº OR MM29", SAF "AdvEve" ➩ ↓ risk "Hº OR MM29"
2. IN:
a. Lab confirmed C19 <5d
b. ONSET sORs <5d
c. 1 sORs <5d
d. 1rf_sDP:
>60yo
CKD - DM
BMI ≥30
actCA
COPD
serious♡ (HF, CAD or CMP)
3. TIMELINE
- May 6, 2021 = 1st px
- Sep 10, 2021 = 50% of 1550 ➩ D29 = intAN
- Oct 2, 2021 = Last px
- Nov 4, 2021 = ƒ-up 29
Saturday 14.05.22 at 14h00 BE
LFMC, JJFM, AAQC
2021 NEJMe - MOVe-IN, randomized Trial of Molnupiravir or PLA in pxs Hº w_C19 (arribas) [RCT]
SOC = standard of care ⏤ SAF = safety ⏤ ARF = acute respiratory failure ⏤ GCP= Good Clinical Practice ⏤ disch = discharge
1. 2021, NEJMe, 15 countries ➩ db_pla_p-2/3_RCT ⏤ 300 (i218 VS c75) ⏤ Oct2020-Aug2021(ƒ-up included) ➩ P⃣ inH°TTO, lab-confirmed C19, SYMPonset ‘D10 OR before randomization’’ I⃣ MOLNU 200,400 OR 800mg BID 5d (1:1:1:1 ratio) C⃣ PLA O⃣ pOC: SAF + RECOVERY (alive ± ‘noHº OR disch D29’) ➩ NO clinical benefit
2. Need therapies safe, effective + easily for pxs C19, MOLNU: NHC ➩ error viral RNA replication.
3. IN: Adult, C19+, SYMPon D10 ⏤ EX: CIpx C19 (ARF [IMV, NIMV,HFNC,ECMO], Shock, MOD), sevIMMUNO↓ , PLT <100k OR transf <5d.
4. SOC = TTO w_ remdesivir +/OR glucocor = permitted ⏤ NO other immunoMODUL.
5. Conduced w_GCP ➩ protocol online ➩ safety performed by indep data monitoring committee.
6. C19 S&S + oxygenation status were assessed daily d_TTO + at days 10
7. The co-primary EP = safety + sustained recovery.
8. Safety = rates_AdvEve reported d_the safety ƒ-up period (from random through 14 days aft_end.of.TTO)9. Sustained recovery = participants alive + ‘not Hº OR medically ready for Hº_disch through D29’.
Saturday 21.05.2 at 23h15 BE
LFMC, AAH,GSQA, AAQC
2022 NEJM - Protection by a Fourth Dose of BNT162b2 against Omicron in Israel (Bar-On) [R] .pdf
1. 2022, NEJM, IS ➩ OBS ⏤ 1.2M ⏤ Jan10-Mar2 ➩ P⃣ adults ≥60yo I⃣ 4rd dose aft_8d C⃣ a. 3rd dose b. Internal (4rd dose 3-7d) O⃣ cases + sC19 ➩ ↗️ 4rd dose 🙂
2. TIMELINE
* D1 = January 1 = recruitment
* D3 = January 3 = vax campaign
* D10 = January 10 = not started yet = start day
* February 18 = sC19 end of confirmed
* July 30 = approval 3rd dose (elderly)
* D? = March 2 = end of study
* D? = March 4 = extracted info = C19 (+)
3. EX: died before beginning + no age & sex + C19 (+) by PCR or antigen + 3rd dose ← approval + abroad d_all the study + ←10D→ in IS + OTHER type of VAX
4. DEFINITIONS:
* CASES = C19 (+) PCR or ANTIGEN
* sC19 = NIH definition = >30RR, <94%, <300 = 14d aft_C19 (+)
5. More DATA = “VAX = dates + brands (1st, 2nd, 3rd, 4th)” + “DEMOGRAPHIC = age, sex, demo group (Jewish, Arab, etc)”
6. 1st group (4ta dosis) = D8 - D14 aft_VAX = WEEK 2
7. INTERNAL GROUP = not confirmed ‘C19 or severity’ BECAUSE it was early
Saturday 28.05.22 at 14h00 BE
LFMC, AAQC
2022 NEJM - Fourth Dose of BNT162b2 mRNA Covid-19 vaccine in a Nationwide Setting (Magen) [R].pdf
HSA = Health security agency ⏤ Clalit Health Services = CHS
1. 2022, NEJM, IL ➩ obs ⏤ >182k (every group) ⏤ Jan3-Feb18, 2022 ➩ P⃣ ≥60yo w_3rd dose I⃣ 4th dose C⃣ not 4th dose (yet) O⃣ 5pOC (INF + SYMP + Hº + sC19 (NIH) + MM) ➩ ↗️
2. Ω (Nov2021 1st appeared) ➩ ↑ despite successful mass-vax campaigns
3. SA + UK = Ω ‘↓virulent’ ∆ ➩ ALTHOUGH… large No INF = concerns overwhelm
4. Pfizer, Moderna, Astra = limited protection Ω
5. WANING IMMUNITY = 10w AFTER 3RD DOSE (Lab + real-world studies) [2022, UK HSA, effectiveness of 3rd dose ⏤ Ferdinands, et al, 2022, MMWR, waning 2-dose and 3-dose effectiveness
6. Early booster countries = IL , UK, USA ➩ received booster several months earlier
7. IL = 4th dose = Jan3, 2022: hrPxs = ≥60y + immunodeficiency = AT LEAST 4m aft_3rd dose = 700k received 4th dose
8. USA = CDC ↓ ‘interval 3rd-4th’ FROM 6m TO 5m
9. Magen et al, took POTENTIAL CONFOUNDERS into account
10. Jan3-Feb18, 2022 (Ω predominant) ➩ CHS = 4.7M = 1/2 IL population = digitalized since 2000 = repositories include all data
11. IN ➩ ≥60yo + CHS at least 1y + elegible to 4th dose (>4m from 3rd dose) + PCR C19 (-)
12. EX ➩ HC workers, long-term facilities, confined at home, interaction w_HC systems (previous 3d, would be included in CONTROL) + DUE TO MISSING DATA <1% (BMI, population sector or residency area were taken)
13. OC ➩ pOC 5 (INF + SYMP + Hº + sC19 (NIH) + MM) = periods ‘D7-D30 + D14-D20’ ➩ ADDITIONALLY: TO “gradual build-up of immunity and evaluate the similarity of the study groups“ = PCR during each day of ƒ-up
14. OVERLAP of >44k = initially ‘control’ and then were rerecruited as ‘intervention’ aft_receiving 4th doseStudy Design
Saturday 11.06.22 at 14h00 BE
LFMC, AAQC
2022 NEJM - EPIC-HR, oral Nirmatrelvir for hr, nHº Adults (Hammod) [RCT]
1. EPIC-HR ▶ NEJM, 2022, USA105, BG30, SA28, BR26, IN19, MX18, UA17… +14c ▶ ph2-3_db_RCT ➖ >2.2k (>1.1k nirma+rito 🆚 1.1k pla) ➖ July-Dec2021 ▶ P⃣ nonHº_symp_unVax_C19 + ’rf_sDP’ (high risk) I⃣ nirma+rito C⃣ pla O⃣ pOC: ‘Hº or MM28’ (mod_ITT) within 3d aft_sympON (EX: mAb ‘at random’) ➕ sOC: = pOC within 5d = ➩ 89% ↓’r_sDP’
2. 💊 300mg nirma + 100mg rito (pharmacokin enhancer)
3. VIRAL LOAD ➩ ↓ nirma+rito (d5 TTO): IF within 3d aft_sympON
4. ⛔AdvEve ➩ similar I&C = any + serious + discontinuation (23vs24%, 2vs7%, 2vs4%) ➩ Dysgeusia + diarrhea = ‘+Freq’ I⃣
5. hr_sDP = 🧓🏼± 🚬± underC (🫀🐷 CA) ➩ latter: 2x sDP + 5x MM = wo_underC (Thakur, SciRep 2021)
6. SAFE & EFFECTIVE TTO ➩ ⤹ ‘sDP, Hº, MM’ + ↓ ttCR + ↓ transR
7. mAb LIMITATIONS ➩ need of admin&monit IN HCsett + variants efficacy?
8. NIRMA MECHS ➩ targets Mpro (essential in replication cycle) ➩ METABOL = CYP3A4 (rito ⊖ it)
9. 💊SAFE DOSE (500nirma + 100rito, BID, x10d) ▶ SIMULATIONS ➩ BID 300 nirma + 100 rito = achieves&maintains 🩸 PLASMA [] 5-6x the in vitro 90%
10. IN ↔ EX
11. PROCEDURE ➩ tech sys for randomization ➩ stratified by: geographic region + receipt mAbs (manufacturer: Pfizer for nirma, HeteroLabs for rito, 🧑🏽🦯 by Pfizer)
12. EFFICACY ➩ ⤹ = groups ➩ adjusted to: sex, race, BMI, serology, viral load, underC, rf
13. sEP = quantif_viralLOAD 👃🏼swab (d1, 3, 5, 10, 14)
14. SAFETY ➩ ⛔ A. AdvEve = d_±aft_TTO (≤d34) B. Serious AdvEve C. AdvEve leading to DISCONTINUATION
Saturday 18.06.22 at 14h00 BE
AAQC
2022 JAMA - I-TECH, Efficacy of Ivermectin TTO on Disease Progression Among Adults W_ Mild to Moderate C19+Comorbidities (lim) [R].pdf
MY: Malaysia; cp = clinical progression; NPRA: National Pharmaceutical Reg Agency
1. I-TECH: JAMA, 2022, MY ▶ mc_ol_RCT ➕ 20 Hº ➕ May-Oct, 2021 ▶ P⃣ ≥50yo, lab C19, ≥1 comorbidities, mild-mod (WHOcp scale 2-4) I⃣ iver 0.4mg/Kg x 5d + SOC C⃣ SOC O⃣ pOC: proportion of pxs sDP ➩ sOC: ratesMV, ICUadm, Hº_MM28, AdvEve ➩ ✖
2. MY ▶ 95% mild + 5% severe
3. Early clinical studies on IVER = methodological weaknesses
4. COL+ARG= NO effect on RESOLUTION + Hº ➩ MAcochr = NO evidence for C19 TTO or PREV
5. EX:

Saturday 25.06.22 at 14h00 BE
AAH, SGQA, AAQC
2022 JAMA - I-TECH, Efficacy of Ivermectin TTO on Disease Progression Among Adults W_ Mild to Moderate C19+Comorbidities (lim) [R].pdf
MY: Malaysia; cp = clinical progression; NPRA: National Pharmaceutical Reg Agency
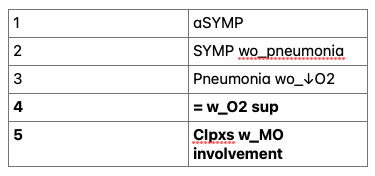
1. CLINICAL severity (WHO equivalence), stages:
2-3 mild & mod = WHO 2-4
4-5 severe = WHO 5-9
2. RANDOMIZATION + DATA COLLECTION ➩ REDCap used ➕ 1:1 ➕ central, computer-generated ➕ permuted block sizes 2 to 6
3. INTERVENTION ➩ IVER was imported as off-label, approved by NPRA, Maxford Healthcare (Indian industry WHO certified) ➩ DOSE = nearest 6mg or 12mg (D1 = AFTER randomization ⏤ D2-D5 = 4 doses)
4. OUTCOME MEASURES ▶ pOC = PROP px_pSD = need to maintain SpO2 ≥95% (stages 4-5) ▶ sOC: t_pSD, H+_MM28, MVrate, ICUadm, H+_LOS ▶ D5 = new assessment = SYMPresol + changes LABresults + Xray ▶ S_AdvEve: TERMINOLOGY V 5.0 ▶ ALL OC captured from RANDOM ⏤ DISCH or D28enroll (whichever EARLIER)
5. SUBGROUPS ▶ C19vax + age + CLINstaging + d_ILLNESS + comorbidities
Saturday 02.07.22 at 15h00 BE
JCAS, AAQC
2022 NEJM - CLASSIC, restriction of Intravenous Fluid in ICU pxs W_ septic shock (Meyhoff) [RCT]
1. CLASSIC ▶ NEJM, 2022, DEN, NOR, SW, SWIT, IT, CR, UK, BE (8 sites) ▶ INT_stra_pg_ol_RCT ➕ >1.5k (31 ICU) ➕ Nov2018-Nov2021 ▶ P⃣ SS• I⃣ restrictive C⃣ standard O⃣ pOC: MM90 ▶ sOC: days alive wo_LIFEsupp + day alive and ooH
2. IN ▶ adults (≥18yo), ICU, SS• (suspORconf INF, lact≥2, vpORiono infusion, 1L 💉 solution before), <12h shock
3. EX ▶ SS• >12h, pregnant, no consent, life-threatBleed, burn >10%
4. AdvEve of fluids:
* worsening KI ➩ ICM 2016 - CLASSIC, Restricting VOL in SS• after initial mm, “mc feasibility” (Hjortrup)]
* ARF (8-10) ➩ ICM 2017 - Conservative mm or deResus S• ± ARDS ƒ resus phase, srMA (siversides, Ferguson) ➩ CCM 2014 - Simplified sevS• protocol: RCT of mEGDT in Zambia (Andrews) ➩ JAMA 2017 - Effect of earlyResus on inHº MM among S• + ↓AP, RCT (Andrews)
* ↑r MM (11) ➩ NEJM 2011 - MM aft_fluid bolus African children w_sINF (maitland)
Saturday 09.07.22 at 15h00 BE
EACQ, AAQC
2022 JAMA - Association of Music Interventions With Health-Related Quality of Life (mccrary) [srMA].pdf
UNSD = United Nations Sustainable Development; CENTRAL = Cochrane Central Register of Controlled Trials; ICTRP = International Clinical Trials Registry Platform
1. 2022, JAMA, DE ▶ srMA ➕ <780 (26 studies) ➕ Jul30, 2021 ▶ P⃣ clinical + healthy populations I⃣ SF36 + SF12 ← → music exposure (making ± listening) C⃣ control (wo_music exposure) O⃣ HRQOL ➩ ↗️ with music
2. HRQOL concept = an individual’s or group perceived physical and mental health over time = wellbeing
3. UNSD goals = To ensure healthy lives and promote well-being for all at all ages
4. LISTENING + MAKING music ➩ increasingly ADVOCATED even by WHO ➩ MAGNITUDE of music effects on HRQOL is UNCLEAR ➩ TYPES and DOSES as well
5. SF-36 ➩ most widely used instrument in health ➩ strong validity + sensitivity + reliability ➩ used in several studies ➩ short form = SF-12 = both consistent
6. DATABASES (4) = MEDLINE, EMBASE, Web of Science, and PsycINFO ➕ CLINICAL TRIALS (3) = CENTRAL, ClinicalTrials.gov, ICTRP
Saturday 16.07.22 at 15h00 BE
GATL, EACQ, SGQA, AAQC
2022 NEJM - LOVIT, Intravenous Vitamin C in Adults w_S• In the ICU (Lamontagne) [RCT].pdf
UNSD = United Nations Sustainable Development; CENTRAL = Cochrane Central Register of Controlled Trials; ICTRP = International Clinical Trials Registry Platform
1. 2022, JAMA, DE ▶ srMA ➕ <780 (26 studies) ➕ Jul30, 2021 ▶ P⃣ clinical + healthy populations I⃣ SF36 + SF12 ← → music exposure (making ± listening) C⃣ control (wo_music exposure) O⃣ HRQOL ➩ ↗️ with music
2. HRQOL concept = an individual’s or group perceived physical and mental health over time = wellbeing
3. UNSD goals = To ensure healthy lives and promote well-being for all at all ages
4. LISTENING + MAKING music ➩ increasingly ADVOCATED even by WHO ➩ MAGNITUDE of music effects on HRQOL is UNCLEAR ➩ TYPES and DOSES as well
5. SF-36 ➩ most widely used instrument in health ➩ strong validity + sensitivity + reliability ➩ used in several studies ➩ short form = SF-12 = both consistent 6. DATABASES (4) = MEDLINE, EMBASE, Web of Science, and PsycINFO ➕ CLINICAL TRIALS (3) = CENTRAL, ClinicalTrials.gov, ICTRP
Saturday 30.07.22 at 15h00 BE
AAH, SGQA, ALAC, AAQC
2021 JAMA - PROSPECT, Effect of Probiotics on Incident VAP in CIpxs (johnstone) [RCT]
1. 2022, JAMA, CA+USA+SA ▶︎ mcRCT ➕ >2500 ( I⃣ >1.3k C⃣ >1.3k) ➕ <6y (Oct2013-Mar2019) ▶︎ P⃣ CIpxs + MV I⃣ L. Rhamnosus GG (1x1010) C⃣ PLA O⃣ pOC = VAP ➩ SAME ⏤ sOC = 20 (5 are IMP) ICUaINF + diarrhea + antiMICROBI use + ICU LOS, H+ LOS + MM ➩ SAME
2. IN: adults >18yo ➕ MV <72h
3. EX: had already received MV >72h ➕ immuno↓ (HIV w_CD4 < 200, cIMSUPP meds, chemother last3m, prior organTransplant, absN count <500) ➕ rENDOVASC INF ➕ sAcPAN ➕ percutENTfeeding + palliation + other or current TRIAL
4. IMPORTANCE ▶︎ TTO + PREV: INF + INFLAMM condit + AI cond ▶︎ gut barrier + ⊖ pathogenic bac + modulation
5. DATA UNCLEAR FOR safety and use ▶︎ RCT, >2500, newborns 👶🏼, India, L. Planetarium + fructooligosacharide ↓r S• + ↓🫁 TI 🙂 ▶︎ srRCT ↓aTB-assoc diarrhea 🙂 BUT not for Cdiff 🙁 ▶︎ REPORTS = POSSIBLE HARM ⛔️
6. RCT ▶︎ 20% INF ↓ (srMA 2016) + 25-30% ↓ VAP (srMA 2016 + ∑ 2020) + cost effective
7. GL (2016) ▶︎ individualized use of PRObiotics (documented safety + benefit) 🤔
8. Allocation 1:1 ➩ parallel-group ➩ STRATIFIED (center + ADM status med, Sg, trauma) ➩ block sized 4 or 6 by WEB-BASED randomization 💻 ➩ unblinded pharmacists randomized pxs & prepared product
9. ADMIN DURATION ▶︎ 60d OR disch OR Lactobacillus was isolated (sterile site or ‘cultured as SOLE or PREDOMINANT from nonSterile’) ▶︎ 100th capsule cultured 🔍 LIMR at McMaster U., Hamilton, Ontario = to CONFIRM fidelity of viable probiotics + integrity of PLA ✩ 10. RECORDED 📜 ▶︎ baseline DATA (demoGRAPH, illSEV, lifeSUPP)➕ daily DATA (prodADMIN, PNEUprevStrat, other coINTERV)➕ culture ➕ INF ➕ diarrhea ➕ LOS ➕ MM
Saturday 06.08.22 at 15h00 BE
GATL, MKFA, AAQC
2021 JAMA - Association of Social Support With Brain Volume and Cognition (Salinas) [R]
ADRD: Alzheimer disease and related disorders, lev_: levels, m&p: mental and physical
1. 2021, JAMA, USA ▶︎ restros, cross-ectiona (prosCollData) ➕ >2k ➕ 1997-1999 (original) - 1998-2001 (offspring) ▶︎ P⃣ participants of Framingham (2 groups: original + offspring) I⃣ MRI + NeuroPsy C⃣ ✖︎ O⃣ Q: social support ↔ cognitive resilience (ADRD vulnerability + cognition) ➩ pOC: global measure of cognitive function
2. IN ▶︎ in Framingham
3. EX ▶︎ dementia + stroke + other Neuro conditions
4. COGNITIVE RESILIENCE
- modification of TOTAL 🧠 volume’s ↔ w_COG
- SMALLER ß estimates = ↑ cogResilience
- General capacity to REMAIN COGNITIVELY UNIMPAIRED despite age- OR ADRD- related PATHOl changes.
- Condition = individual has OBSERVED cogPerf better than EXPECTED given their brain’s structure.
5. LOW CognResil ▶︎ CognPerf is ‘= OR ↓’ than EXPECTED
6. Loneliness + social isolation ▶︎ ↑r ‘COGNdecline + ARDR pathol’
7. CognResil-enhancing FACTORS ▶︎ educational attainment ➕ phys&mental activities ➕ socialRelat measures
8. Clinicopathol study (Lancet Neurol, 2006) ▶︎ Rush Memory and Aging Project ▶︎ 2006, LANCETn, ? ▶︎ longCoh ➕ 89 ➕ ? ▶︎ P⃣ dementia-free elderly I⃣ social networks C⃣ ✖︎ O⃣ Q: social networks ↔ AD & level CognFunct ➩ pOC: CogFunc ➩ >socialNetw size (baseline) ↔ >lev_CognFunct (regardless: neurofibrillary tau + globalADRD neuroPathol)
all INDEPENDENT of: m&p activities, depressSYMP and ChroMed_conditions
although a STRUCTURAL_aspect, resembles a FUNCTIONAL_aspec OF socialRelationships = LISTENER AVAILABILITY
MEASURE derived of 3Q (a. who feels close with, b. No w_whom felt at ease&able to talk, c. How many see monthly)
9. PROMISING strategy to ↓ ADRDr + ↑ neuroCog health (cognitive resilience pathways) = TARGETIN social relationship factors EARLIER IN LIFE
10. All supportive functions 🆚 narrower subsets of SOCIAL SUPPORT ▶︎ are both equally IMP? ➩ composite: socialSupp_measures + ARDS_vulnerab
11, HYPOTHESIS (“we proposed that”) ▶︎ specific forms of SocialSupp ENHANCES cognResil ➩ ↓ clinicalExpress of lower TOTAL CEREBRAL VOL, because:
Neural networks across many CORTICAL + SUBCORTICAL 🧠 regionsProposed preclinical ADRD MRI markers to only SINGLE or SUBSEt OF REGIONSUse of TOTAL 🧠 VOL would ↗️ representation of HETEROG IN ADRD neuropath.
Saturday 13.08.22 at 15h00 BE
AAH, AAQC
2022 NEJM - LOVIT, Intravenous Vitamin C in Adults w_S• In the ICU (Lamontagne) [RCT]
pOD: persistent organ dysfunction – VP: vasopressor – LST: life sustaining therapy – WW: worldwide – ALI: acute lung injury – RANDO: randomization – b_: before
1. 2022, NEJM, FR+NZ+CA ▶︎ p3_mc_RCT ➕ >850 pxs ( I⃣ >430 C⃣ >430) ⏤ 35 ICUs ➕ Nov2018 - Jul2021 ▶︎ P⃣ S• pxs I⃣ VitC 50mg/Kg, every 6h x 4d (96h) C⃣ PLA O⃣ pOC: ‘MM or pOD ➩ ↘️
2. IN ▶︎ >18yo ➕ ICU<24h ➕ provenORsusp INF (mainDx) ➕ w_VP
3. EX ▶︎ VitC_contraIND➖open-label ➖ exp_MM f_48h ➖ withdraw_LST f_48h (see Sup)
4. sOC ▶︎ D_wo_OD, MM 28D + 6m ➕ QOL 6m ➕ SOFA ➕ BIOMARKERS (lactate, IL1ß, TNFalfa, thrombomodulin, angiopo2) at D3 + D7 ➕ OD D2,3,4,7,10,14, 28 ➕ APACHE
5. EPIDEMIO ▶︎ 1/3 or 1/2 death in H+ ➩ 11M deaths WW / y
6. THEORY ▶︎ VitC:
antiOX effects = ↓ tissINJ
Not synthesized in humans = lowLEV in ICUpxs ∑
7. EBM ▶︎ VitC:
w_Hydroc+Thiam = 1 center study spurred interest
Subsequent RCTs = NO benefit
inContrast = RCT: ’S• + ALI’ w_hDose VitC (same) = ↓rMM28 ∑ ↗️
MA = overall evidence = VitC in S• is of LOW CERTAINTY
8. METHODS ▶︎
Trial design = who, where, protocol, ethics + funded, responsibility, eligibility&collection, consent (deferred) + draft, accuracy & completeness & fidelity (to protocol)Pxs = IN, EX, detailsRando & TTO = 1:1, web-based (permuted blocks), unaware + VitC dose (mixed 50-ml dex5% or NS, d_30-60min q6h, x4d), infusion preparation (pharmacists out of clinCare) + glucocor&thiamine at discretion of tto_teams, data_coll by staff, phoneITW by centralMGM_team 6m a_RANDO, pOC completed at 6m ITW if discharged b_d28.
Saturday 20.08.22 at 15h00 BE
AAQC
2022 LANCET - RECOVERY Baricitinib in pxs admitted to hospital W_ C19 [RCT]
BAR: Baricitinib, uc: usual care, RUXO: ruxolitinib, TOFA: tofacitinib, ictrp: International Clinical Trials Registry Platform
1. RECOVERY (baricitinib):
2022, LANCET, UK ▶︎ MA ➕ >8k (8RCTs) ➕Feb-Dec2021 ▶︎ P-HºC19w_BAR I- BAR&uc C-uc O-pOC: MM28 ➩ ↗️ BUT not < preTrials
2. IN: RCTs in HºC19 w_BAR in MEDLINE, Embase, MedRxiv, WHO ictrp ➖ 2yo + suspORconf_LAB_C19 + noHIS_r_“if they were to participate in the trial” (opinion of attendPhys)
3. EX: <2yo ➖ eGFR<15 ➖ diaORhemofil ➖ N<0.5x109 ➖ actTBC ➖ preg&brea
4. sOC: (2)
a. ttD_H+,
b. cOC of iMV(ECMO included)øMM,
5. subsid_clinOC: (3)
a. iMVøNIV
b. ttSuccCess_iMV (within + SS = 48h)
c. dialøhaemofil
6. safeOC (5)
a. cau-specMM
b. majCardArrhy
c. thromEven
d. majBleeEven
e. otherINF
5. #: 8RCTs = 3BAR, 3RUXO, 2TOFA = 6 fully published
6. R: (3)
a. BAR ↓28MM by 13%
b. ↑prob_DISCHalive28
c. ↓prob_prog_cOC (‘iMVøMM’)
Saturday 27.08.22 at 15h00 BE
AAH, ±ALAC, AAQC
2022 LANCET - RECOVERY Baricitinib in pxs admitted to hospital W_ C19 [RCT]
• RECOVERY: 2022, LANCET, UK ▶︎ MA ➕ >8k (9RCTs) ➕Feb-Dec2021 ▶︎ P-HºC19w_BAR I- BAR&uc C-uc O-pOC: MM28 ➩ ↗️ BUT smaller than prevTrials
• IN: RCTs in HºC19 w_BAR in MEDLINE, Embase, MedRxiv, WHO ictrp ➖ 2yo + Hº pxs + suspORconf_LAB_C19 + noHIS_r_“if they were to participate in the trial” (opinion of attendPhys)
• EX: <2yo ➖ eGFR<15 ➖ diaORhemofil ➖ N<0.5x109 ➖ actTBC ➖ preg&brea
• sOC: (2)
a. ttD_H+,
b. cOC of iMV(ECMO included)øMM,
BAR = baricitinib, STAT = signal transducers and activators of transcription, AI = artificial intelligence, ttR = time to recovery, CRF = case report form,
1. EBM
- BAR > sC19 > acutInflProcess > ARF > MV or MM
- Corticosteroids: ↓r MM
- IL-6 blockers: ↓r MM
- JAK inh (poten tto of sC19)
- AI: ↓ endocyto C19 virus into LUNGS = BY INHIB ‘AP2-assoc_protKin1’ & ‘cyclin G assoc Kin’
2. THEORY
- Indications: RA + atoDerm (UK licensed)
- 4 families = JAK 1, 2, 3, TYK2 > ICsignalling > cytok + ITF (both extraCell)
- JAK inhib = PREVENT downstrePhospho > activ STAT (JAK - STAT pathway)
- JAK-STAT pathway = MEDIATES many citok (IL6 included) > IT IS RAISED in sC19
- mod INH TYK2 > Genetic DATA > CAUSAL LINK ‘TYK2 - lifeThreaC19‘
3. Image explanations
4. Related EBM
- ACTT-2: BAR+REM vs REM > pOC = ttR > ↗️
- NEJM 2021 (Kalil): BAR > pOC = MM28 > prob ↗️
- FDA > EUA 2020 > C19 Hº w_O2-iMV-ECMO
5. RECOVERY = dexa + HQC, lopi-rito, azithr, toci, convaPlas, colch, ASA, casi-imde = 177 H+ UK = 159 for BAR
6. CRF = demog + respSupp + coMORB + suitabilityTTO + VAX + TTOavailab
7. RANDOMIZATION: 1:1 + unstratified + allocation concealed > SOME PXS = BAR unavailable OR DEFindicated_or_DEFcontraindic = EX from the randomized comparison8. DOSE = 4mg x 10d = dose reduced for: <60GFR or u_probenecid + <9yo = RISKS: discretion of managPhysi (rINF + GIperforat)
Saturday 03.09.22 at 15h00 BE
AAH, AAACC, AAQC
2020 JIC - Automated pupillometry to assess CAR (Quispe-Cornejo) [R]
• 2022, JIC, BE ➖ prosObs + 92 (52 septic) + Jan2017-Mar2019 ➖ PICO:
- P: ICU pxs (septic - nonSep)
- I: PU + TCD (Mxa)
- C: no
- O: presentCAR
• IN: adults + <48h
• EX: ocular DISøSx + NervSys DIS + arryth + ECMO + supra-aorArterio + noAL
1. S + Sø = causes of ICUadmission + disabilities
2. NEUROimp in S = not IntraCranSource or primBrainInjur needed.
3. S brain alts = DYS BBB + NEUROtransm + neuroInflamm + microcir
4. Autopsia = CEREBRAL ISCHEMIA = cerebral hypoperf <––> neuroDYSF
5. iCAR —> brainHYPOPERF
6. CAR =capacity to MAINTAIN ‘adequ + stable’ CBF in RESPONSE to ≠stimuli:
- change in AP
- CO2
- local: metabolic activation
7. Injured pxs = iCAR
8. iCAR = SABD + l-t COG impairment
9. REMAIN UNKNOWN in CAR physiology TO OPTIMIZE pxOC >> changes in CBF as response to CPP ø MAP
10. IF CAR overridden = CBF is pressure-depend
11. MECHS = myo + neuro + metab + ANS
12. methods to measure ANS = HRV + Pupillometry >> parasymmp = 3rd cranial n >> sympathetic = cervSpin nerve
13. Data collection: demographic + comorbidities + APACHE + concomThe + bloodGas + biolo&hemody
Saturday 10.09.22 at 15h00 BE
JBO, AAQC
2022 NEJM - Blood-Pressure Targets in Comatose Survivors of cardiac arrest (Kjaergaard) [RCT]
• BOX trial: 2022, NEJM, DK ➖ db_ii_2cen_RCT2x2fd + 789 px + Mar2017-Dec2021 ➖ PICO
- P: ohCA in ICU
- I: map63 (ol_INT: liberal vs restrictive O2 –– subordinate random Tº a_24h)
- C: map77
- O: pOC = all_cauMM90 Ø H+DISCH(cpc 3-4)90 >> NO DIFF
• IN: ≥18yo + ohCA (cardiac cause), ≤20min chestCompr + remainedComa (no response to verbalComm)
• EX: unwitnessAsys + susp_acIC_BLEEDorST
• sOC: NSE 48h + allCau_MM + MoCA_3m + mRankin_3m + CPC_3m >> NO DIFF
—————————————————————
ohCA: out-of-hospital CA, pP: perfusion pressure
1. we need a good perfusion pressure (no BP targets known) >> aim is to deliver pP to briain, heart, kidneys
2. hypothesis: lowering AFTERLOAD may facilitate cardiac recovery and POSSIBLY SURVIVAL
3. Careful with AdvEve w_vasoactives (cathecol) >> we use them to increase MAP >65
4. 3 RCT: compared 2 maps + used surrogate EP + R:neutral _ NONE powered (clinEP + safety)
5. BOX: BLOOD pressure and oxygenation targets in post resuscitation care
6. REPORTED: O2 target (separated) + Tº (not included)
7. All done according to Danish legistations
Saturday 08.10.22 at 15h00 BE
JCAS, AAACC, AAH, ALAC, AAQC
2021 JAMA - Steps per Day and All- Cause Mortality in Middle-aged Adults (Paluch) [R]
CARDIA: Coronary artery risk development in young adults,
1. BS: 2021, JAMA, USA (CARDIA: Alab, Ilinoi, Minnes, Calif) ➖ prospCoh + >2k + 11y ➖ PICO:
- P: clinical + population settings (black + white) (middle age)
- I: accelerometer (2005 - 2006):
• volumen = low, moderate, high step groups
• intensity = 30-min stepRate + time at ≥100step/min
- C: no
- O: allC_MM
• IN: all CARDIA population
• EX: see CARDIA
—————————————————————————————
1. Regular physical activity has HEALTH BENEFITS: CVD + DM +
CA + QOL
2. Number of steps = MEANINGFUL METRIC + easy to use (wearable devices) + feasible to monitorize in a population -wide level
3. National GL >> do NOT include STEP COUNTS because there are not enough prospective studies showing ≈ clinOC (MM)
4. EBM:
- Prospective: made in older, few in middle age + age
- sr: device-measStepVol ≈ allC_MM (older)
- NHANES + NORWEGIAN: start to take middle ages
- PhyActiv GL: need subgroups = age, race, sex (all ≈ dailySteps + health)
- USA NationalGL: phyActi recommended is ≥150min/wk of mod-vigor intensity
5. 2021 Wang: 400k = a. accumulating mod-to vigor-intensi ≈ MM b. vigorous-inten (compTO mod) has GREATER ↓MM
6. Epidemiologic: self defined walking pace ≈ MM
7. REcent: volume rather than intensity ≈ MM
8. STROBE used
9. CARDIA: >5K + 18-30yo + 1985-1986 + race, sex, age, education + in-person + years 2, 5, 7, 10, 15, 20, 25, and 30 visits
10. Retention rates AMONG SS: pxs in the sudy / year = 91%, 86&, 81%, 79%, 74%, 72%, 72% 71% (with the years expressed above)
Sunday 16.10.22 at 15h00 BE
ALAC, AAQC
2022 LANCET - Acute respiratory distress syndrome. causes, pathophysiology, + phenotypes (Bos) [r]
dli: diffuse lung inflammation, QT: chemotherapy, dad: diffuse alveolar damage,
1. ARDS = dli + edema >> Pphy complex + ACTIV + DYSREG overap&intera pathw: injury + inflamma + coagul (lung and syste) >> MV can exacerbate
2. we need ↑reg anti-inflamm + ↓reg proinflamm
3. INTRO: 10% ICU admiss (2016) + ↑awareness d_C19 (↑ incidence) +
4. TRADITIONAL CAUSES ➩ INF vs non-INF (direct & indirect)
- INF: ++sepsis (++lungs)
- non-INF: pancraet + sTrauma w_Sø + TRALI + aspiratGASTRICcont
- not SPECIFIC: -ol, smoking, air pollutants
- Genetic hetero? (small) >> Hp-2 (haptoglobin variant) 60% in EU ancestry = ↑r ARDS in sepsis.
5.SINCE 2000 causes HAVE changed = <traumatic (MV, cryst, tarnsf) = <iatrogenic
6. 2018 = ‘e-cig + vaping' (young) + drug-induced (QT), ImmT + vPneu (++ ‘SARS-CoV + H1N1 + MERS-CoV + SARS-CoV-2’)
7. PATHPHY ➩ challenging to understand = incomplete = ‘animals + humans (mechanistic)’ study limitations >> multiple overlapping + interacting INJURY RESPONSE pathways (inflamm + coagu: lung & syst) - DEGREE of INVOLVEMENT
- CLASSIC: +++dad (ALTHOUGH only 45% post-mortem) = N alveolitis + hyaline memb depositi (++bilatPneum - +daHH)
- proteinaceus deposits in ALVEObasemen membr (alveo-cap barrier) = KEY ROLE vs uncertain generalization (selected instancrs of ARDS)
8. epith&endoth barriers INJURY:
- EPITHE damage = epith activation w_ADHESION MOL + PROinflam + PROCOAG pathways + paracell permeab + epithe necrosis (➩DAMP activation = amplify proInflamm signalling ) = alveolar flooding
- Type II cell injury = surfactant impairment
- Concom injury + Glycocalix shedding = proInflamm
- Concom injuty ➩ Anticoag molec shedding - ALL previous ➩ FIBRIN formation = hyaline membrane formation.
TIME MANAGEMENT
48:43:15
Round: 3 13:06:17 appraisal and new hintsRound: 2 17:03:04 DevelopmentRound: 1 18:33:93 JC intro
Saturday 17.09.22 at 15h00 BE
AAACC, EACQ, AAH, MKFA, MIMC, AAQC
2022 NEJM - Blood-Pressure Targets in Comatose Survivors of cardiac arrest (Kjaergaard) [RCT]
ohCA: out-of-hospital cardiac arrest, VP: vasopressor
1. PROTOCOL: guidelines at phys_discretion >> Tº maintained 36º (ohCA) >> pxs w_’MV + SED (propo-fenta)’ >> Tº control w_’surface cooling ø IV devices’ >> Tº was ↑ (normoTº) + SED was ↓ >> Neuro_OC by attendPhys
2. TRIAL INT: unaware of BP targets (clinical staff, invest, pxs, OC_assessors) >> invasive AP monitoring >> goal 70mmHg = ↑10% or ↓10% = low-target (63) + high-target (77)
- Module providers (Core Lab) NO OTHER intervention in the trial >> pxs arrived ↪︎ ICU ↪︎ randomized b_invAP_monit >> 2 measures wo_blinding = CVP ø PAC
- PROTOCOL: 3-stage approach = CVP 10 + NE + DOPAMINE (10ug/Kg/min) >> max dose of VP captured (electronic ICU DB) >> used VP-INOTROPIC score = ↑score is ↑degree of support
3. OC MEASURES:
- pOC = composite (MM ø H+DIS_90)
- CPC for H+DIS = 3-4 = severeDISAB ø coma ø vegetativeState
- If DISCH alive w_CPC3-4 = event WERE recorded AT time of discharge
- sOC = MM90, ttRRT, NSE48h a_rando, MOCA 3m, mRankin 3m, CPC 3m. (6)
- Rankin = range 0-6 = worst_6 (death) – best_0 (no symp)
- MoCA = range 0-30 = ≥26 is normal
- Assessment CPC + Rankin + MoCA = trained ReseaPers
- Due to C19 = telephone OR reviewH+charts = MoCA was not done
4. AdvEve = bleed + INF + arrhy + electrORmeta abnor + AKI w_RRT + seizures (6)
5. STATS: 6mMM was 33% >> power 0.8 - 0.9 >> planned = 800 w_f-up 3m >> groupDIFF in BP + NE + VP-INO = repeated measures variance model >> pOC model used = sOC (ttRRT + all-cau_MM90)= proportion-hazard >>
Saturday 22.10.22 at 15h00 BE
ALAC, AAH, MKFA, AAACC, AAQC
2022 JAMA - High-Dose Dexamethasone + Oxygen Support Strategies in ICU Pxs W_ Severe C19 Acute Hypoxemic Respiratory Failure (COVIDICUS)
IMV: invasive mechanical ventilation; DAWLS: days alive wo_LS
TIME MANAGEMENT
Round: 2 49:35:25 SCOPE + allRound: 1 16:34:11 overview
Saturday 29.10.22 at 15h00 BE
MAL, AAQC
2022 LANCET - Acute respiratory distress syndrome. causes, pathophysiology, + phenotypes (Bos) [r]
AM: Adhesion mole; ARVD: acute right ventricular dysfunction; PLDM: proinflammatory lipid-derived mediatios (PG + LT); da: disease-associated; pa: pathogen-associated; OF: organ failure
TIME MANAGEMENT
01:09:37
Round: 2 02:52:39 commentsRound: 1 01:06:45 refresh last JC + current JC
1. A JC is an academic session where we go through a scientific article for 1 hour.
2. It takes place every Saturday.
3. Its purpose is to understand and discuss relevant elements about the content taking interactive and pedagogic notes (highlighting, underlining and using other learning resources) about the content.
4. We generate further appraisal, identify the opportunities of learning and formulate some potential research questions.
5. We write down the key-points of every session and publish them on our website
6. The article for the next session is posted one week in advance the must-read JC channel of our DISCORD server.
October, 2022
September, 2022
Glossary (most used)
↑ = increase, ↓ = decrease,↗️ = improve,↘️ = worsen, 𝗘𝗫 = exclusion, 𝗜𝗡 = inclusion, ★ = recommendation(s), 🗣 = suggestion(s), critILL = critically ill, DX = diagnosis, h_LOS = Hospital length of stay, icu_LOS = ICU length of stay, inc_ = incident, MA = metaanalysis, mc = multicentric, MM = mortality, MM90 = mortality at 90 days, pxs = patients, pOC = primary outcome(s), sOC = secondary outcome(s), SS = survival, w_ = with, wo_ = without, RCT = randomized controlled trial, sr = systematic review, yo = years old.
Brief scope glossary
- 𝙄𝙌𝘾 BS 🟰 𝙄𝙉𝘼𝘼𝙌𝘾 ᴮᴼ brief scope ↩
- Y, J, C ➖ T ➕ N ➕ t ➖ P I C O: ↩
- year (Y), journal (J), country (C) ➖ type of study (T) ➕ number of patients/sample (N) ➕ time (t) ➖ population (P),
intervention (I), comparison (C), outcome (O, OC).
Complete glossary here